Q) What is the Surgery in FAP patient after colectomy for ampullary adenoma Stage IV
a)Classic Whipple
b) Pancreas preserving duodenectomy
c) Transduodenal excision
d) endoscopic excision
Answer is free for all
6000+ High-Yield MCQs & Explanations – NEET SS MCH
Q) What is the Surgery in FAP patient after colectomy for ampullary adenoma Stage IV
a)Classic Whipple
b) Pancreas preserving duodenectomy
c) Transduodenal excision
d) endoscopic excision
Answer is free for all
Q) Polyposis associated with least risk of colon cancer
a) Familial juvenile polyposis
b) Peutz Jeghers syndrome
c) Cowden syndrome
d) Cronkite Canada syndrome
Ans visible for premium members
Q) Most common delayed complication of loop gastrojejunostomy
a) anemia
b)) gastric reflux
c) stricture
d) malignancy
Ans visible for premium members
Q) Risk factor for CA GB are all except
A. Multiple polyp
B large gall stone >3 cm
C PSC
D pigment stone same risk as cholesterol stone
Ans visible for premium members
Q) True statement regarding GIST is (AIIMS 2019)
a) 80% of GIST arise from stomach
b) ILeal GIST is resistant to Imatinab
c) Leiomyosarcomas do not express CD 117
d) Prognosis of GIST does not depend on the site of lesion
Answer is in the button below and can be seen only when you are a premium member and logged in
Q) Feature on USG that has the highest sensitivity to predict thyroid carcinoma consistently across studies? ( #Head and Neck Onco)
a)Microcalcifications
b)More tall than wide
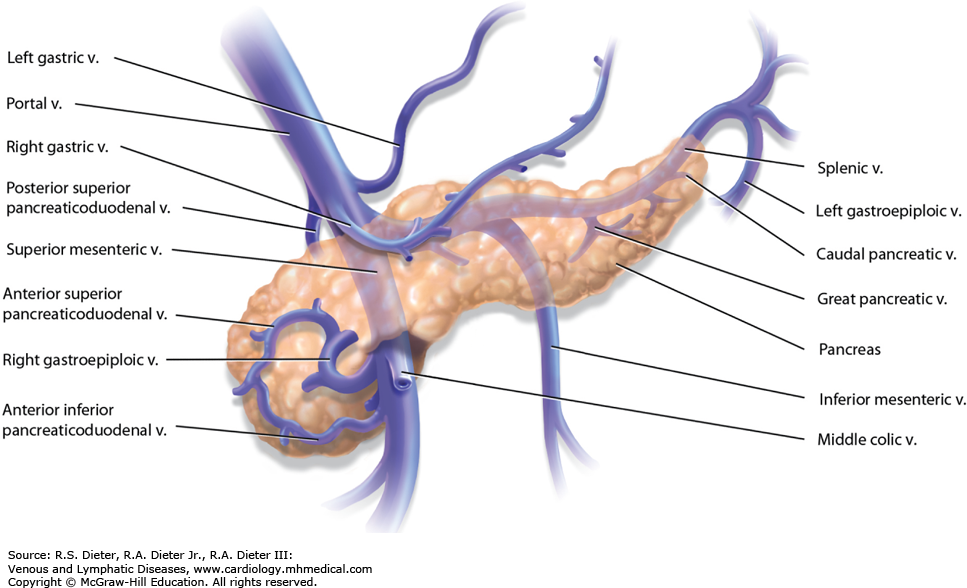
Q) Right gastroepiploic vein drains into
A. Splenic vein
B. Left gastric vein
C. Portal vein
D. Superior mesenteric vein
ANswer is free
Q) Most common cause of pseudoachalasia is ?
(a) Benign tumors of esophagus
(b) Chagas disease
(c) Caustic injury
(d) Adenocarcinoma of cardia