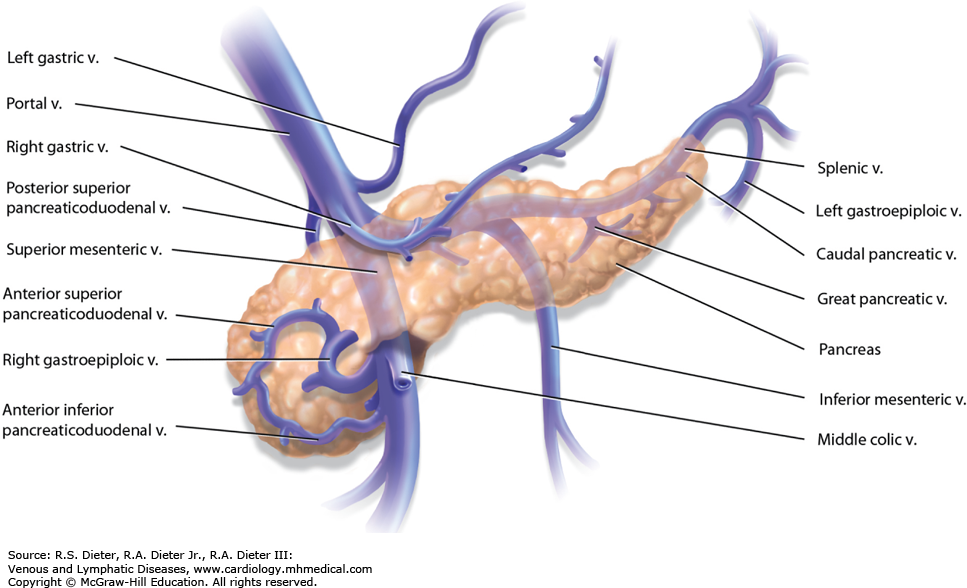
Q) Right gastroepiploic vein drains into
A. Splenic vein
B. Left gastric vein
C. Portal vein
D. Superior mesenteric vein
ANswer is free
D SMV The right gastroepiploic vein is a significant blood vessel located in the abdomen. It runs parallel to the right gastroepiploic artery and is an essential part of the venous drainage system of the stomach. Originating from the greater curvature of the stomach, this vein receives blood from various branches, including the short gastric veins. As it continues its course, it eventually joins with the superior mesenteric vein, contributing to the portal venous system. Understanding the anatomy and function of the right gastroepiploic vein is crucial for medical professionals in diagnosing and treating related conditions, ensuring proper circulation and overall digestive health. The right gastroepiploic vein is essential in many surgical procedures: