Respiratory failure is the cause of death in the early phase (7 days). The pulmonary manifestations of pancreatitis include atelectasis and acute lung injury where as infective complications are the cause of death in late phase.
Q) Which of the following is true about ameloblastoma
a) It is seen in children below 5 years
b) It is the most common odontogenic tumor
c) Mandible is the most common site
d) It is highly malignant
Ans
c Mandible is the most common site
It is the 2nd most common odontogenic tumor. It is locally invasive and can cause severe deformity. It is seen in middle age group and not children.
Mandible is the most common site of origin seen in 80% cases. It is slow growing but it remains locally aggressive with high rates of recurrence.
Given the choices above, c is the most probable one.
Ameloblastoma is a benign, slow growing, locally invasive odontogenic tumor. It is the second most common odontogenic neoplasm. It accounts for 11% of all odontogenic tumors.
Q) An infant presents with duodenal atresia. Which of the following is true about this condition?
a) It is the most common GI atresia
b) It presents soon after birth with non bilious vomiting
c) Pre natal detection of duodenal atresia is common
d) Gastro jejunostomy is the procedure of choice to bypass the obstruction
Answer
C-
Commonly detected in the pre natal ultrasound
Duodenal atresia is seen in 1:5000 live births .Most common atresia is jejunoileal (1 in 2000). It is associated with lot of other congenital malformations like Down's, prematurity, biliary atresia etc.
Duodenal atresia can have many stages like duodenal webs, complete stenosis and complete separation.
Mostly (80%) stenosis is distal to the ampulla of vater so the bile coming out from the ampulla goes in the stomach and infant presents with bilious emesis.
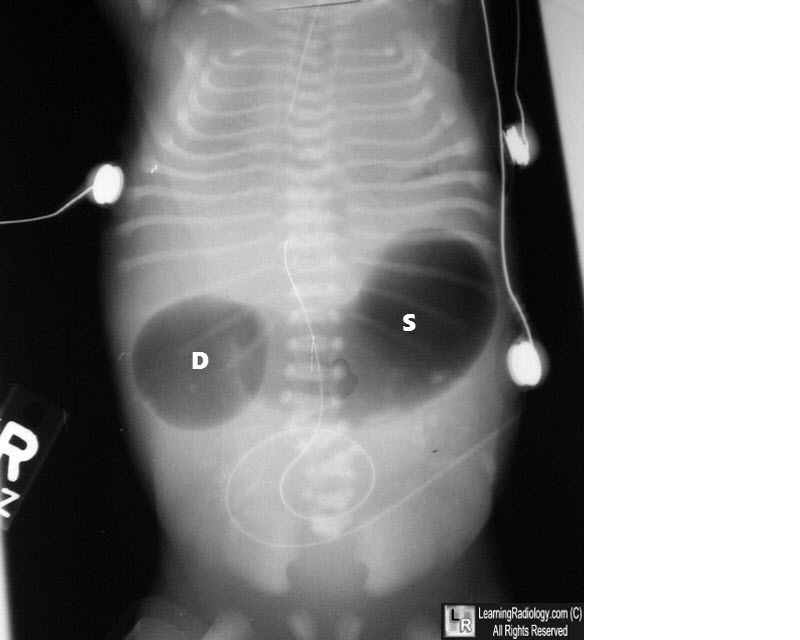
Typical radiographic sign is double bubble. One bubble in stomach and one in duodenum. Ante natal sonography is able to pick up most cases.
Double Bubble
Surgical options include- Duodenoduodenostomy and Duodenojejunostomy.
Another related MCQ to this question is that Double bubble sign is seen in which other conditions
Duodenal stenosis
Annular Pancreas
Atresia of duodenum
Understanding Duodenal Atresia in Infants: Key Facts and Diagnostic Insights
Duodenal atresia is a congenital condition that affects newborns, impacting their gastrointestinal (GI) system. While not the most common form of GI atresia, it is a significant condition that requires early detection and treatment. This article delves into the critical aspects of duodenal atresia, including its symptoms, diagnosis, and treatment options.
What is Duodenal Atresia?
Duodenal atresia is a congenital obstruction of the duodenum, the first part of the small intestine. This condition occurs in approximately 1 in 5,000 live births and is associated with other congenital malformations, such as Down syndrome, prematurity, and biliary atresia.
Prenatal Detection of Duodenal Atresia
Early Diagnosis through Ultrasound
One of the most notable aspects of duodenal atresia is that it is commonly detected during prenatal ultrasounds. Advances in antenatal sonography allow doctors to identify most cases before birth, providing an opportunity for early planning and intervention. The typical sign on ultrasound is a "double bubble" appearance, which indicates the presence of fluid-filled areas in both the stomach and duodenum.
Symptoms and Presentation
Bilious Vomiting After Birth
Duodenal atresia typically presents soon after birth, with one of the hallmark symptoms being bilious vomiting. In around 80% of cases, the obstruction is located distal to the ampulla of Vater, allowing bile from the liver to mix with stomach contents, leading to greenish, bilious emesis.
Associated Congenital Conditions
Infants with duodenal atresia may also present with other congenital anomalies, such as Down syndrome, heart defects, or other gastrointestinal malformations like jejunoileal atresia, which is actually the most common type of GI atresia (occurring in 1 in 2,000 live births).
Types of Duodenal Obstructions
Stages of Duodenal Atresia
Duodenal atresia can occur in various forms, ranging from partial obstruction, such as duodenal webs, to complete separation of the duodenum. These different forms dictate the severity of symptoms and the urgency of intervention.
Duodenal Webs – Thin membranes that partially block the duodenum.
Stenosis – A narrowing of the duodenum that restricts food passage.
Complete Atresia – A total obstruction where the duodenum is completely separated.
Diagnostic Features
Double Bubble Sign on Imaging
Postnatally, duodenal atresia is diagnosed through abdominal imaging, with the "double bubble" sign being a classic radiographic finding. This sign appears as two distinct gas-filled bubbles—one in the stomach and one in the duodenum—indicating the obstruction.
Treatment of Duodenal Atresia
Surgical Intervention
The treatment for duodenal atresia is surgical, with the goal of bypassing or removing the obstruction. Contrary to some misconceptions, gastrojejunostomy is not the preferred procedure. Instead, a duodenoduodenostomy is often performed to connect the two ends of the duodenum, allowing normal passage of food from the stomach to the intestines.
Post-Surgical Outlook
With early surgical intervention, the prognosis for infants with duodenal atresia is generally positive. Post-operative care is crucial to ensure proper digestion and prevent complications such as infection or malabsorption.
Q) In a 55 year old male with a bleeding peptic ulcer, endoscopy is done. Which of the following findings on endoscopy predicts the highest rate of re bleed?
Previous history of breast cancer if completely treated is not an contraindication of liver transplant. Portal vein thrombosis was earlier considered a relative contraindication but almost all series have shown similar results in patients with PVT than patients without PVT.
IN portal vein thrombosis, inflow to the new liver can me taken in many ways
a) thrombectomy
b) Jump grafts from Superior mesenteric vein
c) Anastomosis have been done from big collaterals
Active tuberculosis can be managed after transplant.
Modified ATT regimens without INH and Rifampicin are being used. Any kind of active substance abuse alcohol, drugs etc are absolute contraindications for liver transplant because the disease will recur.
Acalculus cholecystitis can be both acute and chronic in the absence of stones. Although it can present acutely, acalculous cholecystitis typically presents more insidiously.
Mostly the acute form is recognized and chronic form is called biliary dyskinesia.
Jaundice in acalculus cholecystitis is known to occur because of ischemia and inflammation cystic duct gets obstructed due to edema
Diagnosis
Chronic acalculus cholecystitis is a cholescintigraphy nuclear scan (HIDA) with the administration of cholecystokinin (CCK). After the . A calculated ejection fraction of 35% or less may be indicative of hypokinetic functioning of the gallbladder. An ultrasound of the gallbladder may also be useful. If this shows a thickened gallbladder wall of over 3.5 mm, this may be due to cholecystitis.
Q) In gastric cancer, lymph node station 12 corresponds to
a) Common hepatic
b) Hepatoduodenal
c) Retropancreatic
d) Superior Mesenteric
Ans b
In gastric cancer, lymph node station 12 corresponds to the hepatoduodenal ligament lymph nodes. These nodes are specifically located along the hepatoduodenal ligament and are further subdivided into groups based on their anatomical relationship: along the hepatic artery (12a), along the bile duct (12b), and behind the portal vein (12p)