Q Structures which may be injured in mitral valve replacement are all except
A) Circumflex coronary artery
B) Right coronary artery
C) Aortic valve
D) AV node
6000+ High-Yield MCQs & Explanations – NEET SS MCH
Q) 23 year old male has a degloving injury. Degloving injury is one which involves stripping of which layers?
a) Skin
b) Skin, Subcutaneous fat
c) Skin, Subcutaneous fat and underlying fascia
d) All soft tissue upto bones
Q) 33 year old male is undergoing resection of right lobe of liver Which of the following hemodynamic happens during pedicular clamping in liver transaction?
a) Systemic vascular resistance decreases by 20%
b) Mean arterial pressure decreases
c) Cardiac index decreases by 10%
d) Preload to the heart increases
c- Cardiac index decreases by 10%
Portal triad clamping is done to decrease blood loss during hepatic transaction. With the advancement in techniques in donor resection in living donor liver transplants, many centers are shifting away from this but in most centers this is still practiced.
Q) What is true regarding gastric conduits to be used as esophagus replacement?
a) The right gastric and gastro epiploic arteries can be safely divided to bring stomach to the neck
b) For malignant diseases stomach is the most reliable conduit
c) Stomach has the least incidence of developing reflux esophagitis
d) For benign esophageal strictures stomach is the conduit of choice
Q) A 37 year old lady with history of oral contraceptives undergoes a CT scan for pain lower abdomen which also revealed a solitary 6 cm lesion in segment VI of liver. Triple phase Ct scan shows a lesion which enhances in the arterial phase more at the margins and in the venous phase it moves towards the center. This lesion is :
a) Focal Nodular Hyperplasia
b) Haemangioma
c) Hepatic Adenoma
d) Hepatocellular carcinoma
Answer is C
Hepatic Adenoma is benign neoplasms of the liver. They are associated with
They are diagnosed on the basis of CT scans. Diagnostic features of CT Scan for hepatic adenoma are
Hepatocellular carccinoma shows - Rapid arterial filling with wash off in the portal venous phase
Hemangioma- Peripheral nodular enhancement
FNH- Central scar
Q) Management of multinodular goitre with dysphagia and neck pain in a 35-year-old lady:
Q) Which of the following is true about giant gastric ulcer?
a) 70-80% of these ulcers are malignant
b) By definition giant gastric ulcer is more than 1.5 cm in size
c) Medical therapy can heal 80% of such ulcers
d) They are more common on the greater curvature and invade surrounding organs like spleen, liver etc
Answer for premium members
Q) A 45 year old male sustains 30% burns on both legs and anterior abdominal wall. There was mild inhalation injury associated with it. He initially responded well to treatment with IV fluids, Inj Tramadol and enteral feeding.
Three days after the treatment he is having slight tachypnea (30/min) pulse 110/min and BP 98/60. His temp is 97degree F and some areas of partial thickness have converted into full thickness. He is currently on Inj Magnamycin. His platelets are 70ooo, TLC is 17000 and sugar is 200 mg%. What is the next step in management?
a) Continue same management
b) Upgrade the antibiotic and send a fresh culture from skin
c) Treat it as carbon monoxide poisoning
d) Manage in lines of Acute Tubular Necrosis
Burns management involves critical care, intensive phase and rehabilitation. Loss of skin and eschar formation predispose individuals to gram positive, gram negative and fungal infections.
Q) Risk factor for developing melanoma in a pigmented skin lesion is ?
a) Haemangioma
b) Lentigo maligna
c) Congenital nevocellular nevi
d) Tophi
Q) An infant presents with duodenal atresia. Which of the following is true about this condition?
a) It is the most common GI atresia
b) It presents soon after birth with non bilious vomiting
c) Pre natal detection of duodenal atresia is common
d) Gastro jejunostomy is the procedure of choice to bypass the obstruction
Understanding Duodenal Atresia in Infants: Key Facts and Diagnostic Insights
Duodenal atresia is a congenital condition that affects newborns, impacting their gastrointestinal (GI) system. While not the most common form of GI atresia, it is a significant condition that requires early detection and treatment. This article delves into the critical aspects of duodenal atresia, including its symptoms, diagnosis, and treatment options.
Duodenal atresia is a congenital obstruction of the duodenum, the first part of the small intestine. This condition occurs in approximately 1 in 5,000 live births and is associated with other congenital malformations, such as Down syndrome, prematurity, and biliary atresia.
Early Diagnosis through Ultrasound
One of the most notable aspects of duodenal atresia is that it is commonly detected during prenatal ultrasounds. Advances in antenatal sonography allow doctors to identify most cases before birth, providing an opportunity for early planning and intervention. The typical sign on ultrasound is a "double bubble" appearance, which indicates the presence of fluid-filled areas in both the stomach and duodenum.
Bilious Vomiting After Birth
Duodenal atresia typically presents soon after birth, with one of the hallmark symptoms being bilious vomiting. In around 80% of cases, the obstruction is located distal to the ampulla of Vater, allowing bile from the liver to mix with stomach contents, leading to greenish, bilious emesis.
Associated Congenital Conditions
Infants with duodenal atresia may also present with other congenital anomalies, such as Down syndrome, heart defects, or other gastrointestinal malformations like jejunoileal atresia, which is actually the most common type of GI atresia (occurring in 1 in 2,000 live births).
Stages of Duodenal Atresia
Duodenal atresia can occur in various forms, ranging from partial obstruction, such as duodenal webs, to complete separation of the duodenum. These different forms dictate the severity of symptoms and the urgency of intervention.
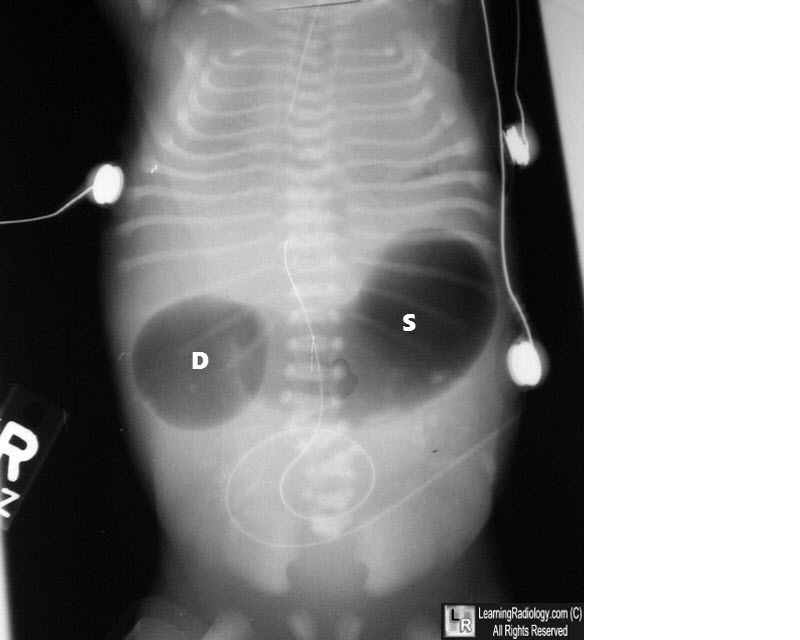
Double Bubble Sign on Imaging
Postnatally, duodenal atresia is diagnosed through abdominal imaging, with the "double bubble" sign being a classic radiographic finding. This sign appears as two distinct gas-filled bubbles—one in the stomach and one in the duodenum—indicating the obstruction.
Surgical Intervention
The treatment for duodenal atresia is surgical, with the goal of bypassing or removing the obstruction. Contrary to some misconceptions, gastrojejunostomy is not the preferred procedure. Instead, a duodenoduodenostomy is often performed to connect the two ends of the duodenum, allowing normal passage of food from the stomach to the intestines.
Post-Surgical Outlook
With early surgical intervention, the prognosis for infants with duodenal atresia is generally positive. Post-operative care is crucial to ensure proper digestion and prevent complications such as infection or malabsorption.